|


|
synonyms: distal radius fracture, Barton's fracture, wrist fracture
Barton's Fracture ICD-10
A- initial encounter for closed fracture
B- initial encounter for open fracture type I or II
C- initial encounter for open fracture type IIIA, IIIB, or IIIC
D- subsequent encounter for closed fracture with routine healing
E- subsequent encounter for open fracture type I or II with routine healing
F- subsequent encounter for open fracture type IIIA, IIIB, or IIIC with routine healing
G- subsequent encounter for closed fracture with delayed healing
H- subsequent encounter for open fracture type I or II with delayed healing
J- subsequent encounter for open fracture type IIIA, IIIB, or IIIC with delayed healing
K- subsequent encounter for closed fracture with nonunion
M- subsequent encounter for open fracture type I or II with nonunion
N- subsequent encounter for open fracture type IIIA, IIIB, or IIIC with nonunion
P- subsequent encounter for closed fracture with malunion
Q- subsequent encounter for open fracture type I or II with malunion
R- subsequent encounter for open fracture type IIIA, IIIB, or IIIC with malunion
S- sequela
Barton's Fracture ICD-9
- 813.40(closed lower end of forearm unspecified), 813.50(open lower end unspecified)
- 813.41(closed Colles Fx), 813.51(open Colles Fx
- 813.42(closed other fractures of distal end of radius alone) (813.52(open other radius alone)
- 813.44 (closed radius with ulna fracture; lower end)
Barton's Fracture Etiology / Epidemiology / Natural History
- Barton's Fracture = a fracture-dislocation of the radiocarpal joint in which the carpus displaces with either a volar (volar Barton's fracture) or dorsal fragment (dorsal Barton's fracture).
- Volar Barton's fracture are more common.
- Barton's fracture's are considered the same as a Smith's type III fracture with a dislcation of the radiocarpal joint.
- Distal radius fractures are the most common fx of UE. 17% of fx/yr.
Barton's Fracture Anatomy
- Distal Radius carries 80% of axial load
- ROM-80°dorsiflexion, 85°palmarflexion, 90°pro\sup,25°radial deviation,35°ulnar deviation
- Barton's 3 column anatomy: Radial column (strong cortical bone), Intermediate column (contains lunate facet and sigmoid notch); Distal ulna column (contains TFCC) (Rikle DA, JBJS 1996;78Br:588)
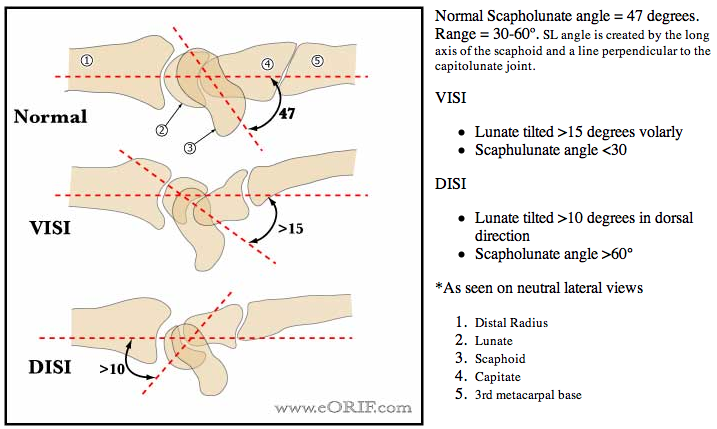
- Radial inclination=23°,radial length=12mm, volar tilt=11°, ulnar variance -0.6mm, scapholunate angle = 60° +/-15°. (Medoff RJ, Hand Clin 2005;21:279)
- Sensory branch of radial nerve becomes subcutaneous 5-10cm proximal to radial styloid in interval between brachioradialis and ECRL. It bifurcates before wrist. Dorsal branch 1-3cm radial to Listers. Supplies 1st and 2nd web spaces. Palmar branch passes within 2cm of 1st dorsal compartment provides sensation to dorsolateral thumb after passing directly over EPL.
- Palmar cutaneous branch of the Median nerve arises from the Median nerve @4-6cm proximal to the volar wrist crease and travels between the FCR and median nerve. Supplies sensation to the thenar area.
- Dorsal cutaneous branch of ulnar n arises deep to FCU, becomes SQ 5cm from pisiform-has multiple branches
Barton's Fracture Clinical Evaluation
- Pain and swelling in wrist
- Document neurovascular exam
- Evaluated for carpal tunnel syndrome
Barton's Fracture Xray
- PA, Lateral wrist films. Normal radiographic parameters: Radial inclination=23°,radial length=12mm, volar tilt=11°, scapholunate angle = 60° +/-15°. Assess ulnar variance, carpal alignment and sigmoid notch conguence.
- Radial length: best measured on true PA radiographs of both wrists for comparision. Draw a line perpendicular to the long axis of the radius intersecting the distal articular surface of the ulnar head. And measure the distance to the tip of the radial styloid. Normal length is 10-13mm
- Signs of DRUJ injury: fracture at the base of the ulnar styloid, widening of the DRUJ space seen on the P/A xray, >20° of dorsal radial angulation, and >5 mm of proximal displacement of the distal part of the radius. (Szabo RM, JBJS 2006;88Am:884)
- 1mm-2mm sagital CT best to view articular depression fx
- MRI if TFCC or scapholunate ligment tears suspected
- CT (3-dimensional) improves recongnition of articular comminution and may aid in pre-operative planning (Harness NG, JBJS 2006;88A:1315).
Distal Radius Fracture Acceptable Reduction
- <2mm articular stepoff
- <5mm shortening
- <10° dorsal tilt
- Surgical indications: radial shortening >3mm, dorsal tilt >10º, intra-articular displacement or step-off >2mm. (AAOS Clinical Practice Guideline, 2011)
Barton'sFractureFx Classification/Treatment
- Displaced volar Barton's fracture = ORIF with volar approach and volar plating. Volar approach is necessary to free and buttress the volar fragment. For fractures with significant dorsal comminution as well consider a locking volar plate or fragment specific fixation. (Konrath GA, JOT 2002;16;578), Benson LS, J Hand Surg 2006;31A:8). Alternatives = closed reduction and percutaneous pinning; external fixation.
- Consider Osteoporosis evaluation and management.
- Colles' Fracture = dorsally displaced fracture of the Barton's generally occuring 2-3 cm proximal to the radiocarpal joint. 90% of Barton's fractures.
- Smith's Fracture = reverse Colles' fracture; may be caused by backwards fall resulting in forced wrist pronation.
- Chauffeur's fracture = intraarticular fracture of the base of the radial styloid. Used to occur then cars backfired while they were being crank started.
Barton's Fracture Associated Injuries / Differential Diagnosis
- Scapholunate ligament tear: 21.5% with intraarticular fracture, 6.7% with extraarticular fracture (Richards RS, J Hand Surg 1997;22Am:772).
- Median nerve injury
- TFCC injury, up to 50% when ulnar styloid fx also present
- Carpal ligment injury:Scapholunate Instability(most common), lunotriquetral ligament
- Tendon injury,attritional EPL rupture, usually treated with EIP tendon transfer
- Compartment syndrome@1%
- Ulnar styloid fracture
- DRUJ Instability
- Galeazzi Fracture: highly associated with distal 1/3 radial shaft fractures
Barton's Fracture Complications
- Malunion = typically loss of radial height, ulnar and volar inclination less commonly inarticular incongruity.
- Nonunion: uncommon except with volar and dorsal plating with extensive sub-periosteal stripping.
- Distal radioulnar joint injury
- Contracture
- Neurologic injury
- Complex regional pain syndrome(CRPS) (2-20%)
- Hardware failure
- Painful Hardware
- Risks of surgery including but not limited to: malunion, nonunion, stiffness, CRPS, nerve or vascular injury, painful hardware, loss of fixation, tendon injury, infection, arthritis, incomplete relief of pain, incomplete return of function and the risks of anesthesia including heart attack, stroke, and death.
Barton's Fracture Follow up care
- Post-Op: Place in volar splint. Encourage active digital ROM, elevation. Consider adjuvant Vitamin C for prevention of CRPS.
- 7-10 Days: remove splint. Place in short arm cast. Consider removable splint with gentle ROM if fixation was extremely secure.
- 6 Weeks: Cast removed. Check xrays. Started gentle ROM exercises. Activity modifications: no heavy manual labor, no contact sports, no lifting >5 lbs.
- 3 Months: Check xrays. If union is complete return to full activities.
- Standard Technique to measure ulnar inclination, palmar tilt, ulnar variance and articular congruity = Kreder HJ, J Hand Surg 1996;21A:532
- Patients may have incomplete return of motion, DRUJ pain and deformity, wrist pain and loss of grip strength. Some permanent disability is not uncommon.
Barton's Fracture References
|
{kind=link}