|
|
synonyms: CTS, carpal tunnel syndrome
Carpal Tunnel Syndrome ICD-10
Carpal Tunnel Syndrome ICD-9
Carpal Tunnel Syndrome Etiology / Epidemiology / Natural History
- CTS = entrapment of the median nerve at the wrist
- pathology=edema and fibrosis, not inflammation
- Risk Factors: female sex, pregnancy, diabetes, rheumatoid arthritis, obesity, alcoholism, hypothyroidism, smoking, aging, exposure to industrial solvents, mucopolysaccharidosis, mucolipidosis.
- Body Mass index and high hand/wrist repitition rate are associated with increased risks of CTS (AAOS CPG 2016)
- Computer use is not related to carpal tunnel syndrome (Andersen JH, JAMA 2003;289:2963).
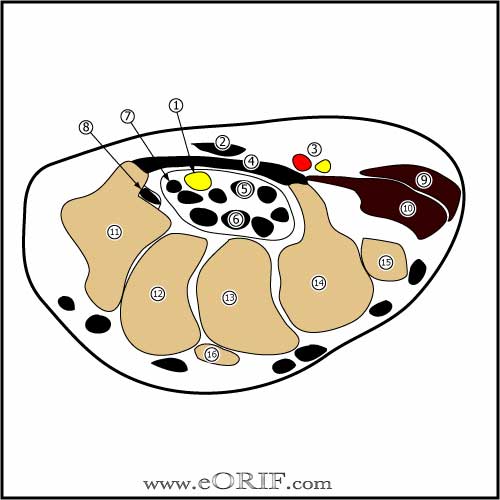
Carpal Tunnel Syndrome Anatomy
- Transverse carpal ligament: thick fibrous band from the the tuberosity of the scaphoid and a portion of the trapezium to the pisiform and hook of the hamate.
- Boundaries of carpal tunnel: volarly=transverse carpal ligament; Radially=scaphoid tuberosity and trapezium; Ulnarly=pisiform and the hook of the hamate; Dorsally=carpal bones and the deep volar radiocarpal ligament and volar interosseous ligaments
- Contents of carpal tunnel = median nerve, 4 flexor digitorum superficialis tendons, 4 flexor digitorum profundus tendons and flexor pollicis longus
- Motor branch of median nerve has many variations; can branch off extraligamentous, subligamentous, transligamentous etc. (Lanz U, J Hand Surg 1977;2:44)
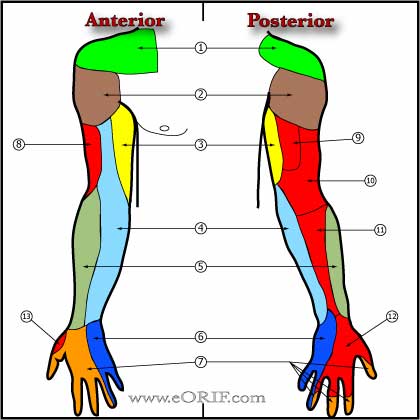
- Palmar Cutaneous Nerve: typically arises from the radial side of the median nerve 5cm proximal to the radial syloid and passes distally just under the FCR tendon. It passes through the transverse carpal ligament radial to the longitudinal axis of the ring finger to supply sensation to the palm. (Hobbs R, J Hand Surg 1990;15A:38) Injury can lead to painful neuroma.
- Kaplan's Cardinal Line = a guideline for locating the recurrent motor branch of the median nerve. Recurrent branch is located at the intersection of a line drawn along the ulnar border of the middle finger, with a line drawn between the radial aspect of the thumb web space in abdcuction and the pisiform.
Carpal Tunnel Syndrome Clinical Evaluation
- Initial:thumb, index and middle finger numbness and tingling.
- Intermediate: wrist and hand pain, night pain and numbness.
- Late: severe compression leads to thenar muscle atrophy and weakness.
- Symptoms may be exacerbated by: driving, reading, typing, prolonged grasping.
- Durkins compression test: (most sensitive and specific )direct compression of median nerve at the carpal tunnel causes paresthesias within 30 seconds.
- Phalens test: hands held in forced maximum flexion for 60 seconds, numbness or tingling in radial digits within 60 seconds is indicative of carpal tunnel syndrome. Sensitivity =40-88%, Specificity = 81% (Kuschner SH, Orthopedics 1992;15:1297).
- Tinel's sign= taping over a peripheral nerve causes sensation of tingling in the distribution of that nerve. Most commonly refers to tapping median nerve as it passes through the carpal tunnel causing tingling in median nerve distribution. Sensitvity = 25-75%, specificity 70-90% (Katz JN, Ann Intern Med 1990;112:321)
- Opponens pollicis muscle strength testing. Weakness in the ability to hold thumb and small finger pads together.
- Semmes-Weinstein monofilament exam.
- Static discrimination is abnormal when >6mm
- Moving two-point discrmination is abnormal when >5mm.
- Note
Carpal Tunnel Syndrome Xray / Diagnositc Tests
- P/A and lateral views of the wrist typically normal.
- EMG/NCV criteria=Sensory latencies (DSL)>3.2ms (most sensitive), motor latencies(DML)>4.2ms. Typical findings: increased insertional activity, positive sharp waves, fibrillations at rest, decreased motor recruitment, complex repetitive discharges. Definitions for conduction delay etc are on p 487 of AMA guides to Impairment 6th ed.
- EMG conduction delay: distal motor latency >4.5ms for 8cm study; distal peak sensory latency >4.0ms for 14cm distance; distal peak compound nerve latency >2.4ms for 8cm study. (AMA Guides 6th ed.)
- EMG conduction block: drop in abductor pollicis brevis CMAP of >30% when wrist stimulation is compared to palm stimulation. (AMA Guides 6th ed.)
- EMG Axon loss: fibrillations and positive sharp waves in the APB. CMAP of <4mV recorded from APB with palm stimulation. (AMA Guides 6th ed.)
- CTS can be diagnosed based on history and clinical evaluation alone. EMG indicated for patients in which the diagnosis is in doubt. (Graham BA, ASSH Annual meeting 2006).
Classification / Treatment
- See AAOS AUC/orthoguidelines.
- Conservative RX=activity modifications, splints, injections. Injections=80% transient relief, 22% symptom free 1yr. NSAIDs(limited efficacy).
- Sugical indications=failed conserv rx, APB atrophy, sensory loss, axonal loss on EMG(<amplitude). >95% of patients will have symptom improvement.
- Patients treated surgical have better outcomes at one year than those treated nonoperatively (Jarvik JG, Lancet 2009; 374: 1074)
- Surgical treatment has greater treatment benefit than conservative care.
- see Carpal Tunnel Release 64721
Carpal Tunnel Injection
- 1.5cc Selestone,1.5cc Lidocaine
- Inject just ulnar to PL at distal wrist crease, needle in to the hub c slight distal angulation.
Carpal Tunnel Syndrome Associated Injuries / Differential Diagnosis
Carpal Tunnel Syndrome Complications
- Failure of decompression (incomplete release of transverse carpal ligament or volar antebrachial fascia, recurrent tenosynovitis, reformation of the flexor retinaculum, postoperative adhesions, intraneural scarring)
- Persistent numbness
- Palmar hypersensitivity
- Proximal pain
- Median nerve palsy (motor branch)
- Wound dehiscence
- Infection
- We discussed the risks of carpal tunnel release including but not limited to: incomplete relief of pain, incomplete return of function, persistent numbness, palmar hypersensitivity, proximal pain, nerve or vascular injury, wound dehiscence, infection and the risks of anesthesia including heart attack, stroke and death.
Carpal Tunnel Syndrome Follow-up Care
- Post-op: Volar splint, NWB
- 7-10 Days: Remove sutures, consider night time splinting. Start gentle ROM exercises
- 6 Weeks: Begin strengthening exercises
- 3 Months:Return to full activities / sport
Carpal Tunnel Syndrome Review References
Greens Hand Surgery |