|




|
synonyms:distal radius external fixation, distal radius ex fix
Distal Radius External Fixation CPT
Distal Radius External Fixation Indications
- Open distal radius fracture
- Displaced distal radius fracture
- Initial management of open fractures with extensive soft tissue loss
- Polytraumatized patient (temporay fixation)
Distal Radius External Fixation Contraindications
- Medically unstable patient
- Ulnar translocation due to unstable DRUJ
- Disrupted volar carpal ligaments/radiocarpal
Distal Radius External Fixation Alternatives
Distal Radius External Fixation Pre-op Planning
- Ligamentotaxis cannot reduce a depressed "die punch" fracture, restore volar tilt, control radial translation or stabilize an unstable distal radioulnar joint.
- Spanning external fixation limits restoration of volar tilt and is associated with increased complications as compared to non-spanning external fixation (McQueen, JBJSB, 1998)
- Consider bone grafting to accelerate bone healing and/or supplementation with internal or K-wire fixation
- External fixation rigidity is increased with: increased rod diameter, wide spread of fixator pins, bicortical pin insertion, more than one plane of fixation and rod placement close to skin/bone. (Behrens F, CORR 1983;178:103)
- Distal Radius Case Card.
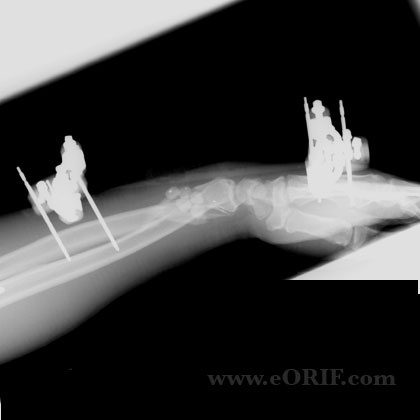
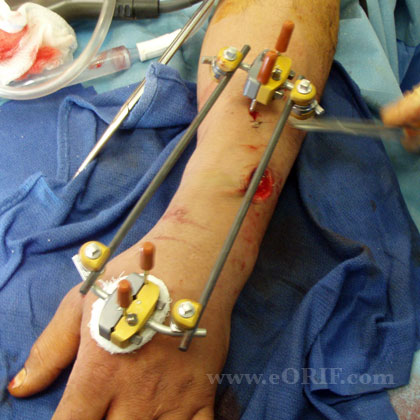
Distal Radius External Fixation Technique
- Sign operative site.
- Pre-operative antibiotics, +/- regional block.
- General endotracheal anesthesia
- Supine position with radiolucent hand table. All bony prominences well padded.
- Tourniquet placed high on arm.
- Prep and drape in standard sterile fashion.
- Two 1-cm incisions over the dorsal radial aspect of the 2nd metacarpal base and radial shaft. Blunt dissection to metacarpal.
- Place 3-mm self-tapping half-pins at a 30°-45° angle dorsal to the frontal plane of the hand.
- 4-cm skin incision10 cm proximal to the wrist joint.
- Dissection down to the radius between the extensor carpi radialis longus and brevis tendons. Between ECRB and EDC is an alternative. Dissection between the BR and ECRL risks the superficial radial nerve.
- Protect the radial nerve.
- Insert towh 3-mm half-pins (1.5 cm apart) at a 30° angle dorsal to the frontal plane of the forearm.
- Confirm pin placement fluoroscopically.
- Apply clamps and bars per manufacture specifications to construct frame.
- Consider augmentation with bone graft, internal fixation, K-wires as indicated. Apply traction with the Ex fix. Consider one 1.6mm/0/062 k-wire through the radial styloid, one or tow from dorsal to palmar to stabilize palmar tilt and one or two transverse subchondral wires for articular support in intra-articular fractures. Then release traction so that ex fix is in neutralization and not distraction.
- Ensure wrist is not distracted. Distraction increases carpal pressures and can lead to CRPS and increased wrist stiffness. External fixation of the wrist should be used as a neutralization device, not a traction device.
- Irrigate.
- Close proximal incision.
Distal Radius External Fixation Complications
- Malunion
- Nonuion
- Infection / Pin tract infection
- Arthrofibrosis
- Finger stiffness
- Tendon rupture
- Compartment Syndrome
- CRPS
- risks of surgery including but not limited to: malunion, nonunion, stiffness, CRPS, nerve or vascular injury, painful hardware, loss of fixation, tendon injury, infection, arthritis, incomplete relief of pain, incomplete return of function and the risks of anesthesia including heart attack, stroke, and death.
Distal Radius External Fixation Follow-up care
- Post-op: Volar plaster splint. Elevation, NWB. Active and passive finger ROM.
- 7-10 Days: Discontinue splint. Clean cutaneous/pin interface with peroxide BID. Active and passive finger ROM.
- Pin-Site Care: there is no significant difference in the incidence of pin-site infection regardless of pin-site care (dry dressings, peroxide, or chlorhexidine impregnated discs). (Egol KA, JBJS 2006; 88A:349)
- 6 Weeks: Remove Ex fix. Consider short arm cast / removeable splint. Active and passive finger ROM.
- 3 Months: Consider occupational therapy if wrist stiffness prevails. Sport specific rehab.
- 6 Months: Return to full activities / sport.
- 1Yr: F/U xrays, assess outcome.
Distal Radius External Fixation Outcomes
Distal Radius External Fixation Review References
|