 |
synonyms: atraumatic sternoclavicular subluxation
Spontaneous Sternoclavicular Subluxation ICD-9
Spontaneous Sternoclavicular Subluxation Etiology / Epidemiology / Natural History
- Generally adolescent or early adulthood. Often related to ligamentous laxity. Reported in patients 10-36 years old.
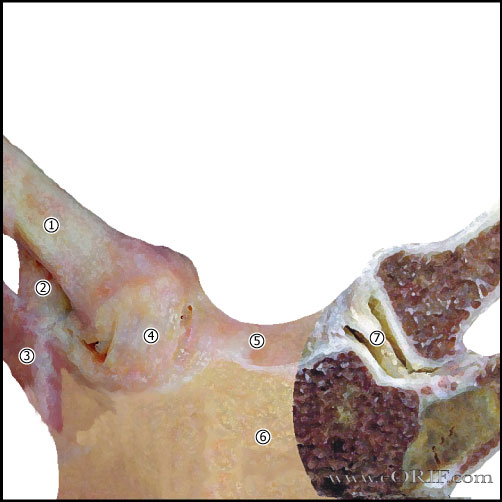
Spontaneous Sternoclavicular Subluxation Anatomy
- 50% of the medial head of the clavicle articulates with the sternum.
- SC joint allows 35° upward motion, 35° arc of A/P motion, 50° of rotation.
- SC joint is a diarthrodial joint.
- The only true articulation between the upper extremity and the axial skeleton.
- The medial clavicle epiphysis does not ossify until 17 or 18. In pts whose epiphysis is unossifed it is impossible to differential between a physeal fx and a dislocation, although fx is much more likely.
- Anterior capsular ligament is the strongest of the SC ligaments and prevents upward displacement of the medial clavicle.
- Costoclavicular ligament (rhomboid ligament): consists of anterior and posterior fasciculus. Anterior fasciculus arises from the anteriomedial aspect of the first rib and insert more laterally on the clavicle. Posterior fasciculus arises lateral to the anterior fasciculus and inserts more medially.
- Intra-articular Disk Ligament: dense, fibrous ligament arising from the synchondral junction of the first rib to the sternum; passes through the sternoclavicular joint, dividing it into two joint spaces.
- Interclavicular ligament: arises from the upper sternum, inserts on superomedial clavicle.
- Posterior capsule most important structure in AP stability of the medial clavicle.
Spontaneous Sternoclavicular Subluxation Clinical Evaluation
- Spontaneous subluxation of the sternoclavicular joint often associated with overhead elevation. May be associated with popping sound / sensation.
- Often painfree.
- Patients may be able to demonstrate subluxation with forward elevation which reduces with lowering the arm.
- Evaluate for generalized ligamentous laxity: ability to touch ipsilateral forearm with the thumb, place palms of hands on floor with knees locked, elbow/knee/MCP hyperextension, patellar instability.
Spontaneous Sternoclavicular Subluxation Xray / Diagnositc Tests
- AP view, apical lordotic view, serendipity view
- Chest xray: If the injured medial clavicle is superior to the normal side the dislocation is anterior. If the injured medial clavicle is inferior to the normal side it is dislocated posteriorly.
- Serendipity View: 40-degree cephalic tilt a/p xray of SC joint. Draw a horizontal line across the image at the superior edge of the normal clavicular head. It the medial clavicle is superior to that line, it is dislocated anteriorly. If the medial clavicle is inferior, it is dislocated posteriorly.
- The medial clavicle epiphysis does not ossify until 17 or 18. In pts whose epiphysis is unossifed it is impossible to differential between a physeal fx and a dislocation, although fx is much more likely.
- CT scan best demonstrates SC instablity.
Spontaneous Sternoclavicular Subluxation Classification / Treatment
- Ice, NSAIDs, shoulder/scapular strengthening exercises. Advance to activity as tolerated. Patients generally can resume full activities without limitations although intermittent subluxations are common. (Rockwood CA Jr, JBJS 1989;71A:1280).
- Surgery rarely beneficial. 100% excellent outcomes with non-op treatment at 8 year follow-up (Rockwood CA Jr, JBJS 1989;71A:1280). Good outcomes have been reported for 3 patients with spontaneous SC instability treated with suture anchor reconstruction (Abidden Z, JSES 2006;15:315).
Spontaneous Sternoclavicular Subluxation Associated Injuries / Differential Diagnosis
Spontaneous Sternoclavicular Subluxation Complications
- Recurrence (generally not functionally limiting)
- Surgical treatment: including noticeable scars, persistent instability, pain, activity limitations
Spontaneous Sternoclavicular Subluxation Follow-up Care
- Advance to activity as tolerated. Patients generally can resume full activities without limitations although intermittent subluxations are common.
Spontaneous Sternoclavicular Subluxation Review References
- Rockwood CA Jr, JBJS 1989;71A:1280
- Lee D, Operative Techniques: Shoulder and Elbow Surgery: Book, Website and DVD, 1e, 2010

- Craig EV, The Shoulder (Master Techniques in Orthopaedic Surgery), 2012
- Williams GR, Operative Techniques in Shoulder and Elbow Surgery, 2010
- Zuckerman JD, Advanced Reconstruction Shoulder (American Academy of Orthopaedic Surgeons), 2007

|